|
July 13, 2020
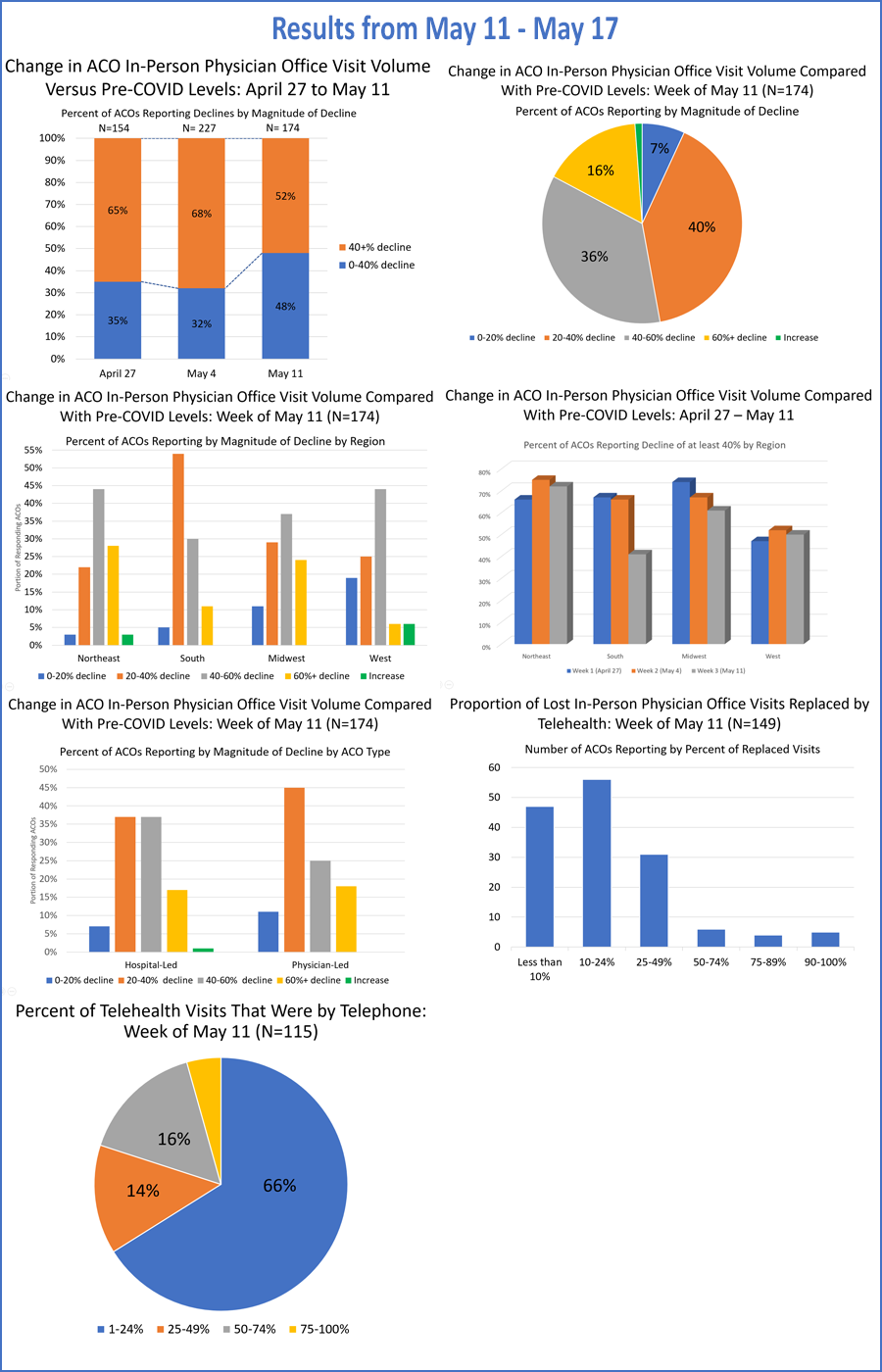
Via www.ncqa.getfeedback.com/r/cF9cai1h/q/0 Re: Public Comment for the Taskforce on Telehealth Policy Dear Leaders of the Taskforce on Telehealth Policy: The National Association of Accountable Care Organizations (NAACOS) appreciates the solicitation of public feedback as the newly formed Taskforce on Telehealth Policy develops its long-term recommendations around telehealth. As the largest association of ACOs, NAACOS works to advance population health-focused payment and delivery models and represents 12 million beneficiary lives through hundreds of organizations participating in models in Medicare, Medicaid, and commercial health plans. This includes the Medicare Shared Savings Program (MSSP), Next Generation ACO Model, Medicare Advantage, and alternative payment models supported by a myriad of commercial health plans. NAACOS and its members are deeply committed to the transition to value-based care. The ACO model is a market-based solution to fragmented and costly care that empowers local physicians, hospitals and other providers to work together and take responsibility for improving quality, enhancing patient experience and reducing waste. Importantly, the ACO model also maintains patient choice of clinicians and other providers. While the origins of Medicare ACOs date back to the George W. Bush Administration, the number of ACOs in Medicare has grown considerably in recent years and includes nearly 550 ACOs in 2020, covering nearly 13 million beneficiaries, almost a fifth of all Medicare beneficiaries and a third in Traditional Medicare. ACOs are leading the way in Medicare’s shift to value-based care and represent the dominant option for providers to participate in alternative payment models. NAACOS has been a long-time supporter of telehealth, which shares the goal of creating a more efficient, more cost-effective health system. These important goals mirror those of our ACO members. We supported the CONNECT for Health Act in both 2017 and 2019. We’ve written the Federal Communications Commission (FCC) on ways to increase access to broadband and telehealth services, which shouldn’t be overlooked as we discuss improving access to health care. We’ve advocated for wider use of remote patient monitoring, another technology that should be considered by this Taskforce’s work. As we discuss below, ACOs are extremely supportive of wider use of telehealth and policies that support that expansion, including improved reimbursement. ACOs feel the technology’s use will stay long after the COVID-19 pandemic ends and should improve patient experience and outcomes. ACOs are currently examining ways to build telehealth into existing delivery platforms. That being said, there are concerns ACOs have expressed regarding telehealth’s expanded use as that could disrupt normal care patterns and affect the methodology on which ACOs are assigned the patients they’re accountable for. Since ACOs are attributed patients based on historical primary care visits, expanded access to telehealth could lead patients to see non-ACO providers that are not part of the patient’s core primary care team, including those with whom the patient does not have an ongoing relationship. This could result in more siloed care and critical health information not flowing back to the patient’s primary care team in the ACO. Additionally, disrupted care relationships could skew ACO attribution, which would change an ACO’s patient population. As the Taskforce develops its recommendations, we hope you urge policymakers to grant ACOs more freedom to use telehealth than tradition, fee-for-service healthcare providers. ACOs are held responsible for the quality, cost, and outcomes of their patients. As such, they hold a responsibility to use telehealth in a cost-effective manner to support whole-person care. If providers take accountability for patients as ACOs do, they should be handed tools to manage their populations, including telehealth, without restraints that are placed on non-accountable organizations. We hope the below feedback is helpful as you work to craft recommendations that foster the long-term use and growth of telehealth. Expanding Telehealth and Its Effect on Total Cost of Care After the COVID-19 pandemic hit, ACOs nimbly moved to adopt telehealth or increase its use within their organizations. According to a survey of NAACOS membership, more than half of ACOs replaced between 10 percent and 24 percent of lost in-person visits with telehealth by early May. About 10 percent of ACOs replaced at least half of lost in-person visits with telehealth in that time. In short, ACOs quickly realized the value of telehealth, if they hadn’t already, and want to see policies put in place that facilitate its use after the current public health emergency ends. While we continue to survey ACOs about their use of telehealth, we’ve heard anecdotally that ACOs continue to deliver between 15 percent and 30 percent of their patient visits via telehealth even in areas of the country not experiencing “spikes” in COVID-19 cases. Some ACOs are moving to adopt a “virtual first” strategy for patient visits and are deploying telehealth across their organizations and systems, both in physician practices and hospitals and with primary care and specialists. ACOs are in the process of better understanding how the technology can be used to meet patient needs and improve care management, while fitting into their economic and care delivery models. NAACOS supports payment parity between in-person and video-based telehealth. Payment parity would incentivize use of telehealth and assist ACOs building out the technological footprint to integrate telehealth into their delivery systems. However, policymakers may want to revisit payment parity in the future as more data becomes available on the economics of delivering a virtual visit and on utilization. Additionally, NAACOS believes audio-only visits should not be reimbursed at the same level as video-based telehealth. Phone-based visits, while necessary during highly unusual circumstances such as a pandemic, deliver less clinical value than video-based visits because of non-verbal communication that is missed, among other differences. Plus, audio-only visits are ripe for overuse. While there is a place for audio-only telehealth, it shouldn’t be reimbursed at the same level and should be limited to certain situations and patients who may not be able to use video-based telehealth. We recommend the Taskforce develop additional guardrails and payment for audio-only telehealth. The Taskforce should not overlook the role of remote patient monitoring. Its use has grown considerably during the COVID-19 pandemic and is an important way to manage patients with multiple chronic conditions. The technology could, for example, be used to keep tabs on the blood sugar levels of diabetic or vital signs of health failure patients. It could be deployed to monitor those recently discharged from the hospital. Remote patient monitoring is often viewed separately from telehealth, which is often defined as a face-to-face visit delivered virtually, but the Taskforce should consider policies that promote its use in its final recommendations. Enhancing Patient Safety and Program Integrity in Remote Care Services In its final recommendations, the Taskforce should allow providers practicing in a value-based payment model, including all ACOs, more allowances to use telehealth than their fee-for-service counterparts. Since providers in these models are responsible for patients’ overall spending and quality, they are hypersensitive to the use of telehealth in ways that will protect against fraud, abuse, and overuse that shows up in peer-reviewed research. To date, research on the effects of increased use of telehealth is mixed in terms of its ability to lower the overall cost of care. As telehealth improves access, it improves convenience and therefore utilization increases too. Little research to date studies telehealth’s use by ACOs, but we know ACOs are penalized for not hitting spending targets and will therefore use the technology in ways that are more efficient and judicious. Comparing ACO spending to the absence of ACOs found the program lowered Medicare spending by $3.53 billion from 2013 to 2017 and saved $755 million after paying shared savings. Therefore, to improve our health care system resilience, we must strengthen and move to payment models like ACOs, which incentivize keeping patients healthy. In the 2018 Bipartisan Budget Act, Congress recognized ACOs’ cost-controlling ability when it pushed for telehealth waivers on patients’ location to ACOs in two-sided risk models who use prospective attribution. The Taskforce should recommend similar policies to provide more waivers for all ACOs, both one-sided and two-sided, beyond those for originating site, including extending patient cost-sharing support, waiving any need to have an established relationship with a patient, allowing the use of certain modalities, and alleviating certain physician supervision requirements. Policymakers should do more to incentivize value-based payment models. The Medicare Payment Advisory Commission (MedPAC) recently recognized the need to move to a payment system that better rewards value. Specifically, MedPAC said ACOs are a vehicle for additional change. NAACOS wholeheartedly agrees and recommends the Taskforce single out ACOs and value-based payment models as a delivery tool to be granted more freedom to use telehealth. Data Flow, Care Integration, and Quality Measurement NAACOS is closely monitoring the impact of COVID-19 on ACO quality improvement efforts. Additionally, quality measurement will be affected and must be reconsidered during the COVID-19 pandemic and in future years. In order for ACOs to leverage telehealth throughout the care and quality ecosystem, all quality measures must be attainable through telehealth as the form of care delivery. As discussed above, telehealth also needs to be made widely available and reimbursed sufficiently. Additionally, remote patient monitoring should be a covered benefit to facilitate accurate measurement collection remotely. Finally, quality measurement and specifications must be retooled to better incorporate the realities of providing care through telehealth. For ACO program quality assessments, the MSSP has applied the extreme and uncontrollable circumstances policy for 2020. Specifically, if an ACO is unable to report quality due to the extreme and uncontrollable circumstance, the ACO’s quality score will be set to the mean quality performance score for all MSSP ACOs for the applicable performance year. However, if the ACO is able to completely and accurately report all quality measures, CMS will use the higher of the ACO’s quality performance score or the mean quality performance score for all MSSP ACOs. While this approach may have been suitable for a natural disaster, such as hurricanes that are more regionally focused, this is not an appropriate policy solution for the COVID-19 pandemic we are currently facing. The avoidance of care by patients and postponement of certain critical services to preserve personal protective equipment (PPE) will have lasting effects on quality. In addition, well visits are also being postponed. As a result, ACOs will struggle to manage patients with chronic conditions and provide proper preventive care during this time. For these reasons, it would not be appropriate to compare performance to quality benchmarks, which were established in previous years. Finally, many ACOs are deploying their quality improvement staff to provide clinical care and assist in triaging patients, detracting them from their more typical quality improvement and care coordination work. As a result, NAACOS does not feel the extreme and uncontrollable circumstances policy goes far enough to mitigate the vast impact of the COVID-19 Public Health Emergency (PHE) on ACO quality measures, and we instead are advocating for CMS and other payers to make all measures pay-for-reporting in 2020. There is value in reporting what data ACOs can during this challenging time. However, ACOs should not be held accountable to typical quality standards during this highly irregular pandemic. We also urge CMS to continue to study the impact of the pandemic on ACO quality in the months and years to come, as it is likely additional policy changes will be necessary in the future. Broader Policy Questions ACOs, like other providers, have become painfully aware of the disparity in technology use borne by patients across the country. Too many patients still lack access to video-based visits because of a lack of broadband access, smartphones or computers, digital literacy, or all of the above. While funding from the FCC has helped support the building of broadband infrastructure, more must be done. The FCC’s Rural Health Care Program, which helps rural healthcare providers purchase broadband and telecommunications services, recently increased its funding by nearly a third, but it now sits at $800 million in money available annually, which is not sufficient compared to what investment is needed. Congress allocated an additional $200 million in telehealth grants for the FCC in a COVID-relief package, but the money quickly ran out. NAACOS takes issue with the narrow definition for eligibility for these programs, which shuts out for-profit entities. NAACOS wrote the FCC asking the commission to reconsider, but the eligibility criteria have not been updated to properly include ACOs and certain other providers that would benefit from this funding. Many of the more than 500,000 ACO clinicians work in independent medical practices, which are overwhelmingly for-profit and therefore ineligible for these FCC programs. In fact, a 2018 American Medical Association survey found 45.9 percent of physicians in the United States owned their own practices. These are often small businesses that have limited cash on hand to support such things as the sudden purchase of equipment to facilitate telehealth and remote patient monitoring. Independent physician offices are valuable players in our health system and need to leverage telehealth for the betterment of community health. Yet they have been excluded from these valuable FCC programs. We urge the Taskforce to recommend the FCC reconsider its eligibility criteria to include them. Conclusion NAACOS appreciates the opportunity to contribute to the Taskforce’s recommendations. The increased use of telehealth from the COVID-19 pandemic is here to stay as providers have woken up to the benefits of telehealth. We hope this is an opportunity to craft polices that cement the increased use of the technology and stand ready to work with Congress, CMS and the broader community to make that happen. If you have any questions, please contact David Pittman, Health Policy and Communications Advisor at NAACOS at [email protected]. Sincerely,
Clif Gaus, Sc.D. |

{kind=link}